Ever wonder why cannabis dosages seem to be vastly different for different patients? These days, deciding whether or not cannabis medicine is right for you may be easier than figuring out exactly how much cannabis is right for you, and in what form. In an industry full of nascent research, confused and unenforced regulation, and misinformation, determining what amount your body needs and the best way to take it can be daunting.
Factors That Affect Dosage
Cannabinoid Profile
Cannabis varieties, strains, and components have widely varied effects, caused by the presence of cannabinoids—the most prevalent being CBD and THC. If you’re new to cannabis, your first step should be familiarizing yourself with cannabinoids and what you can expect from them. If you are on other medications, it’s a good idea to talk to your doctor about any possible interactions. Consuming THC in Utah and many other states requires a doctor’s prescription, so if you are interested in adding THC to your regimen, speak to your doctor about writing you a prescription, or visit a Qualified Medical Practitioner (QMP).
First of all, not all CBD, THC, or full-spectrum product is created equal. By now, even many casual consumers have heard of the Entourage Effect. In this complicated interaction, cannabinoids (from CBD and THC on down to CBG, CBC, CBN, or any of the other hundred or so minor cannabinoids) interact with each other in countless combinations that compound, inhibit, or change the actions of each. CBD and THC are the only cannabinoids that currently have published research detailing their pharmacology, so the effects of the other cannabinoids, either on their own or in concert, are still mostly inferred.
Terpenes
If this weren’t complicated enough, we can’t forget terpenes, which also have their own effects on the body’s physiology, and more importantly, add another hundred plus components to our already complicated web of synergistic combinations. The hundreds of biomolecular components magnify and mitigate each other’s effects, leading to quantifiably different reactions. This synergy is the reason consuming 10 mg of CBD isolate cannot be conflated with consuming 10 mg of full spectrum CBD oil, which in turn is very different than consuming the plant itself.
I am text block. Click edit button to change this text. Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Genetic Differences
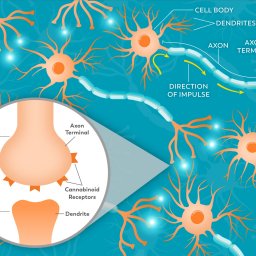
Dosages are also dependent on other interactions, most notably, how your body reacts with cannabinoids. Genetics come into play here in several different ways. First, they determine what types of receptors you have, how many, and where they are located. The more receptors you have, the more chances cannabinoids have to cause an effect. Drug transporters are also genetically controlled, and control how much THC makes it through the blood-brain barrier, and thus its psychoactivity.
These genetic variations are why dosage recommendations start low and then titrate up. Every individual has slight differences that can have a big effect on how their body reacts to cannabinoids. Aside from genetics, tolerance also plays a large role in the dose needed to be effective for an individual. The more an individual consumes THC, the more their receptors are desensitized and retracted. So an individual who has not consumed THC will have more receptors with increased sensitivity than a habitual user. For this reason, doses often have to be adjusted. A 5 mg dose that was sufficient for a new patient may no longer impart the desired effects once that patient has taken it once or twice a day for a sustained amount of time.
Bioavailability
Bioavailability is another factor that affects cannabis dosage. Your lungs will process cannabinoids differently than your digestive tract, which will process them very differently than your skin will. Each route of consumption sends cannabinoids through different absorption and elimination pathways, each of which contributes to different concentrations of them in the bloodstream (and thus their efficacy). You can read our article on different cannabis delivery methods here.

The Biphasic Effect
When taking cannabis, it’s important for patients to start at a low dose, not only to avoid strong psychoactivity, but also because it may be more effective. Cannabis, like alcohol, is subject to the biphasic effect. This means that symptoms may be relieved at low doses, but be amplified if the dose is too high. So while taking a small dose, or even microdosing (which usually means around 2-5 mg/dose), may relieve anxiety and stress, a very high dose might do the opposite, leaving patients paranoid or with racing hearts. Avoiding the latter is important for patients, so it is key to start with a very small dose and increase it by small increments until the desired effects are felt.

Finding The Right Dose
Remember that not all cannabinoids are created equal. Since THC is psychoactive, it’s especially important to begin with a low dose, and increase very slowly in order to get the medical benefits without too strong of a high, which can be uncomfortable for novice consumers. On the other hand, a 2011 study on CBD administered 1,500 mg/day (that’s 1.5 grams!) to study participants for two months, and found it was tolerated well. Other cannabinoids have no scientific data on dosing, but we expect more and more data to contribute to guidelines.
When it comes to settling on the right dosage and consumption method, a lot will come down to the patient and their intent. A first-time cannabis user who needs relief from stress or insomnia will need far less than a patient who takes it regularly for Parkinson’s or Epilepsy. For all users, cannabis advice is to “start low and go slow”.
5 mg is generally a good starting point for either THC or CBD in adults, and patients should give it plenty of time to kick in before taking more. 10 mg is considered a standard dose in the majority of states, with recommended doses going up to 20 mg. In all cases, individual patients need to find the dosage and consumption method that works best for them.
.
References
Agurell, S., Halldin, M. A. G. N. U. S., Lindgren, J. E., Ohlsson, A. G. N. E. T. A., Widman, M. A. R. I. A. N. N. E., Gillespie, H. A. M. P., & Hollister, L. (1986). Pharmacokinetics and metabolism of delta 1-tetrahydrocannabinol and other cannabinoids with emphasis on man. Pharmacological reviews, 38(1), 21-43.
Agurell, S., & Leander, K. (1971). Stability, transfer and absorption of cannabinoid constituents of cannabis (hashish) during smoking. Acta Pharmaceutica Suecica, 8(4), 391.
Brenneisen, R., Egli, A., Elsohly, M. A., Henn, V., & Spiess, Y. (1996). The effect of orally and rectally administered delta 9-tetrahydrocannabinol on spasticity: a pilot study with 2 patients. International journal of clinical pharmacology and therapeutics, 34(10), 446-452.
Ohlsson, A., Agurell, S., Londgren, J. E., Gillespie, H. K., & Hollister, L. E. (1985). Pharmacokinetics and Pharmacodynamics of Psychoactive Drugs. Barnett, G, 75.
Ohlsson, A., Lindgren, J. E., Wahlén, A., Agurell, S., Hollister, L. E., & Gillespie, H. K. (1982). Single dose kinetics of deuterium labelled Δ1‐tetrahydrocannabinol in heavy and light cannabis users. Biomedical Mass Spectrometry, 9(1), 6-10.
Ohlsson, A. J. A. S. L. H., Lindgren, J. E., Wahlen, A., Agurell, S., Hollister, L. E., & Gillespie, H. K. (1980). Plasma delta‐9‐tetrahydrocannabinol concentrations and clinical effects after oral and intravenous administration and smoking. Clinical Pharmacology & Therapeutics, 28(3), 409-416.
Wall, M. E., Sadler, B. M., Brine, D., Taylor, H., & Perez‐Reyes, M. (1983). Metabolism, disposition, and kinetics of delta‐9‐tetrahydrocannabinol in men and women. Clinical Pharmacology & Therapeutics, 34(3), 352-363.